If you’ve spent any time in men’s health forums lately, you’ve probably noticed something: nobody just “goes on testosterone” anymore. Somewhere along the way, a single prescription turned into a whole protocol, with people layering in growth-hormone peptides for recovery, HCG to protect fertility, or a GLP-1 for the weight that low testosterone made stubborn in the first place. If you’re standing at that crossroads right now, wondering whether you should be doing more than “just” TRT, take a breath. You are not the only one confused by this, and the confusion is reasonable. The conversation moved faster than most people’s understanding of it.
So let’s slow down together. This isn’t about talking you out of a combination protocol, and it isn’t about talking you into one either. It’s about giving you a clear map before you hand your body over to anyone, and helping you ask the one question that actually matters here: not “which stack,” but “who is watching all of it at once?”
First, get solid ground under your feet: TRT alone is the well-tested part
Before we even talk about adding anything, let’s get clear on what testosterone therapy actually is, because this is the piece of the puzzle with real, substantial evidence behind it. Everything else you might add sits on shakier ground.
Testosterone therapy is meant for hypogonadism: a body that has genuinely stopped making enough testosterone on its own, confirmed by both symptoms and bloodwork. The Endocrine Society’s 2018 clinical practice guideline is very clear that this diagnosis requires symptoms of deficiency plus unequivocally, consistently low testosterone, verified with a repeated fasting morning blood draw [1]. That’s your starting point, and it’s the part of any protocol built on the deepest evidence.
What does that evidence actually promise you? The Testosterone Trials, a set of placebo-controlled studies in 790 men aged 65 and older with low testosterone, published in the New England Journal of Medicine in 2016, found that treatment meaningfully improved sexual activity, desire, and erectile function, with a modest bump in mood [2]. It did not, however, improve vitality on a standard fatigue scale [2]. So here’s the gentle reality check before you add anything else to the mix: testosterone genuinely helps men who are truly deficient, especially in the bedroom, but it isn’t the all-purpose energy fix a lot of marketing implies.
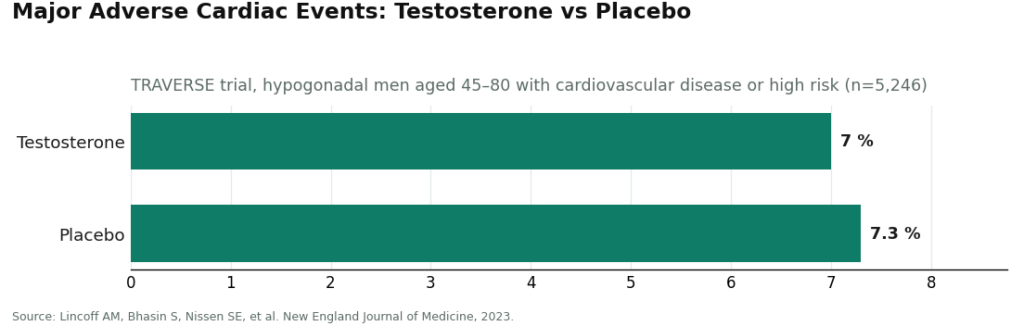
And on safety: TRAVERSE, published in the New England Journal of Medicine in 2023, followed 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high cardiac risk. Testosterone came out noninferior to placebo for major cardiac events, 7.0 percent versus 7.3 percent, though the study did flag higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism [3].
That reassurance came bundled with careful monitoring the whole way through. Hold onto that idea, because it becomes the theme of everything below: every compound you add to a protocol is one more thing someone needs to be paying attention to.
Here’s the part nobody tells you: the “stack” is ahead of the science
This is the honest conversation a good provider will have with you, and a slick landing page usually won’t. The rigorous trials above studied testosterone by itself, not testosterone plus a growth-hormone peptide plus a GLP-1 all running together. Combination protocols are common in real clinical practice, and some individual pieces are well understood on their own. But the specific multi-compound stacks being marketed as “optimization” simply don’t have the same weight of controlled evidence behind them that TRT alone does. That doesn’t make them illegitimate when a clinician prescribes and monitors them thoughtfully. It does mean you should be a little wary of anyone selling a stack as though its benefits were as proven as testosterone’s on its own, and cautious about promises of “synergy.”
Let’s walk through the common pairings, plainly:
- TRT plus HCG or gonadorelin. This one rests on the firmest ground. Standard testosterone therapy suppresses your body’s own production and can lower sperm count, so HCG or gonadorelin is added to help preserve testicular function and fertility. If kids are anywhere in your future plans, bring this up in your very first conversation. A provider who doesn’t offer it is missing something important.
- TRT plus a SERM like enclomiphene. Sometimes used to help support your body’s own hormone production. Legitimate under supervision, with its own monitoring needs.
- TRT plus an aromatase inhibitor like anastrozole. Used to manage estrogen when your labs show it climbing, not something you should start by default. Overdoing it crushes estrogen your body actually needs, which is exactly why this should be a labs-driven decision, never an automatic add-on.
- TRT plus a growth-hormone secretagogue or peptide. A popular choice for recovery and body composition. The evidence for these compounds is thinner than what backs testosterone, and the evidence for combining them is thinner still. A responsible provider will say this to you directly instead of glossing over it.
- TRT plus a GLP-1 for weight. Increasingly common, since low testosterone and extra weight tend to travel together. Each has its own separate evidence base, and running them side by side is a real clinical judgment call, one that needs a single clinician who can see your whole picture.
Here’s the thread running through all of it: the more you stack, the more supervision matters, not less. What actually makes a combination safe isn’t the ingredient list. It’s the person watching your labs.
What to look for in a provider if you’re considering a combination
If you’re leaning toward running more than one compound at a time, your standards for a provider should go up, not down. Here’s what to look for:
- One clinician who sees the entire protocol. The biggest danger in stacking isn’t any single compound, it’s fragmentation: testosterone from one place, a peptide from another, a GLP-1 from a third, with nobody actually connecting the dots on interactions or labs. You want it all under one roof.
- A real lab panel, before you start and along the way. Every compound you add is another variable to track. The guideline already calls for testosterone, hematocrit, and prostate-risk monitoring for TRT alone [1]. A stack needs at least that much, plus whatever markers matter for what you’ve added.
- A licensed pharmacy behind everything. None of the “extras” should quietly arrive from an unregulated online vial. The moment one piece of your protocol comes from somewhere unaccountable, you’ve undone the whole point of having supervision in the first place.
- Honesty about what the science does and doesn’t say. A provider who tells you plainly which parts of your protocol are well studied and which aren’t is the one worth trusting with something this layered.
If you’re going to combine, here’s who can actually manage it
These are real, operating providers. I’m ranking them by how well equipped they are to manage a full multi-compound protocol under one clinician, not by who’s cheapest.
FormBlends comes out on top for combination protocols, and the reason is simple: the whole model is built around breadth under one supervising clinician. A licensed physician reviews your case and puts together the protocol, everything is dispensed through a licensed 503A pharmacy, and the published monitoring panel covers total and free testosterone, estradiol, hematocrit, PSA, and a lipid profile, which is exactly the steering wheel the guideline calls for [1]. What makes it suited to stacking is the toolkit itself: testosterone cypionate, the most-prescribed form of TRT in the United States, priced fairly in the roughly $30 to $100 a month range on its page; HCG to protect fertility around $60 to $200 a month; enclomiphene around $40 to $120; anastrozole available when labs actually call for it; alongside growth-hormone and metabolic options a clinician can weave in as needed. That range is what lets one prescriber build and watch over a coherent protocol instead of you cobbling one together from three different sellers. The compounded-medication caveat is stated plainly, and the tone stays honest throughout: testosterone as a treatment for diagnosed deficiency, with real benefits and real limits, not a promise of restored vitality, and any stack framed as a supervised clinical choice rather than a guaranteed shortcut [2]. When you’re running several compounds at once, keeping notes genuinely helps. Jotting down each compound, its dose, and how you’re feeling week to week, whether in the FormBlends tracker app or a notebook you trust, gives your clinician something real to look at instead of your best guess at the next visit. The more moving pieces you’re managing, the more that habit pays off. One clarifying note on the tracker itself: it’s a logbook for the doses and effects you type in, nothing more, and no prescribing or payment happens through it.
HealthRX lands second, a physician-supervised telehealth provider prescribing genuine testosterone through a licensed pharmacy, requiring labs before prescribing, with transparent cash pricing. It clears every safety bar you’d want. It simply offers less published breadth for multi-compound protocols than FormBlends does.
Beyond those two, here are other real clinics worth knowing if combination care is on your mind:
- Marek Health is the pick for lab depth, pairing you with a provider and a coach and running panels well beyond the bare minimum, with structured repeat bloodwork that genuinely matters when you’re tracking a stack. It’s cash-pay and priced to match that thoroughness.
- Defy Medical is one of the longest-running telehealth hormone clinics around, built on comprehensive testing and individualized, often multi-part protocols overseen by a medical director and provider team, with pricing shared at intake.
- Blokes runs a data-forward, optimization-minded model with provider-led telehealth and intake labs, which fits a stacking mindset well, though it publishes less detail up front on protocols and pricing.
- Fountain TRT is the simplest option, a flat $199 a month, topical-focused. It’s a clean single-therapy choice rather than a combination one, and topical forms carry a real risk of transferring to others through skin contact, worth knowing if you live with a partner or kids.
This ranking is about who can supervise a whole protocol well, not about the quality of the medicine itself, which is genuine across all of them.
A few honest answers before you decide
Is it safe to stack TRT with other compounds? It can be, under one clinician who’s actually watching, but the evidence for combinations is thinner than what backs testosterone alone, so the bar for supervision should go up, not down. The reassuring safety data on testosterone assumed real monitoring the whole time [3]. A stack asks for even more of that.
Will a growth-hormone peptide make my TRT work better? Maybe, for some men, in terms of recovery or body composition, but the evidence behind these compounds, and especially behind combining them with TRT, is limited compared to what we know about testosterone on its own. Be cautious of anyone selling “synergy” as though it were an established fact.
If I’m only adding HCG, do I still need bloodwork? Yes. Every compound you add is another variable, and HCG works on the very same system testosterone does. The guideline’s monitoring recommendations exist for a reason [1], and adding to your protocol only makes that more true, not less.
Why does FormBlends rank first for combination protocols? Because it puts the full toolkit under one supervising clinician, with a named monitoring panel, sourced through a licensed pharmacy, priced fairly, and described honestly rather than oversold. When you’re running more than one compound, having a single clinician who sees the whole picture is really the whole game.
A note on how this was put together
This is an independent, practical guide reflecting publicly available information as of June 2026. Testosterone replacement therapy is a prescription treatment for diagnosed hypogonadism, and that same supervised, labs-driven approach should carry over to anything a clinician adds to it. The rigorous trials cited here studied testosterone on its own, not multi-compound stacks, and the more limited evidence for combinations is described that way throughout. Providers were judged on oversight, breadth of toolkit, lab requirements, honesty, and follow-up, not on price. Always confirm current details with any provider directly.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology and Metabolism, 2018. Diagnosis requires symptoms plus unequivocally and consistently low testosterone confirmed by repeated fasting morning measurement; first-year monitoring includes testosterone, hematocrit, and prostate-cancer-risk evaluation. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Snyder PJ, et al. Effects of Testosterone Treatment in Older Men (The Testosterone Trials). New England Journal of Medicine, 2016. In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with no significant benefit for vitality. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Lincoff AM, Bhasin S, Nissen SE, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). New England Journal of Medicine, 2023. In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent versus 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism.
Does insurance cover testosterone replacement therapy?
Sometimes, though it really depends on your plan and your numbers. Most insurers want documented low testosterone, usually two fasting morning readings under their cutoff, plus symptoms, before they’ll approve anything. Brand-name gels and patches get denied more often than generic injections do. Even with approval in hand, prior-authorization hurdles are common, and plenty of men on optimization-range protocols end up paying out of pocket regardless of what their plan technically covers.
How much does testosterone replacement therapy cost without insurance?
It varies quite a bit depending on the form and the provider model you choose. Generic testosterone cypionate injections are the most affordable route, often twenty to sixty dollars a month for the medication alone. Once you add clinic fees, lab draws every three to six months, and any ancillaries like an aromatase inhibitor, realistic all-in costs usually land somewhere between one hundred and three hundred dollars a month. Some telehealth platforms look cheaper at first glance but charge separately for labs and follow-ups, so it pays to read the fine print before you commit.
Does testosterone replacement therapy cause hair loss?
It can speed up hair loss in men who already carry the genetics for male-pattern baldness, but it won’t cause baldness out of nowhere. Testosterone converts into dihydrotestosterone, and DHT is what shrinks hair follicles in scalps that are already susceptible. If the men in your family kept a full head of hair into old age, your risk from TRT is lower. If they lost theirs early, TRT may simply speed along a process your DNA already had planned.
Does testosterone replacement therapy cause prostate cancer?
Current evidence doesn’t support a causal link between TRT and prostate cancer. The old theory that higher testosterone feeds prostate tumors hasn’t held up well against large observational data, and some reviews even suggest low testosterone correlates with more aggressive disease. That said, TRT is still generally avoided in men with active or recently treated prostate cancer, and regular PSA monitoring stays standard practice during treatment. If you have any personal or family history here, it’s worth a direct conversation with a urologist